Sometimes, I just need to see things for myself.
Many times that teeth are symptomatic, it is secondary to varying degrees of fracture. There are a number of issues that will often accompany a tooth that is vertically fractured. This includes the following findings:
A significant periodontal probing
A gingival swelling not unlike a typical sinus tract in its appearance
Bone loss in a characteristic J shape pattern
But what about when the presentation is not completely in line with the typical presentation. When this happens, by all means, the case has to be visually verified. In the following cases, after following my normal diagnostic steps, I determined that although fracture was a distinct possiblity, I wanted to visualize the damage before making a final determination.
Case #1

Previously treated
Chronic apical abscess
This patient presented with discomfort on the facial aspect of tooth #30. Root canal treatment was initially performed on this tooth in 1987. A sinus tract was present, and after anesthesia, the elusive significant periodontal probing was found. Also, there was little to no bone loss visible on the radiograph. I took the opportunity to make a small incision to expose the facial aspect of #30, confirming the presence of a vertical root fracture.
Case #2

Previously treated
Acute apical abscess
This patient presented with discomfort on the facial of #27. Root canal therapy was performed in 2007. There was no periodontal probing found in this case, and there was no bone loss evident on the radiograph. After surgical access, a narrow trough of bone loss was visualized surrounded by intact buccal plates. After removing the granulation tissue, a vertical root fracture was confirmed.
Case #3
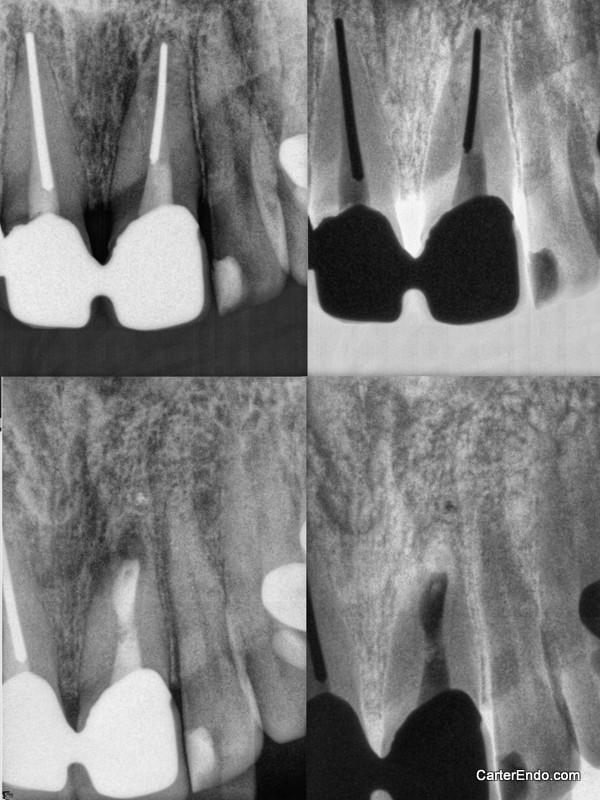
Previously treated
Chronic apical abscess
The patient presented with discomfort in the maxillary anterior after a traumatic incident. An isolated swelling over the apex of tooth #9 was also seen. There was a suggestion of bone loss towards the mesial aspect of the apex on tooth #9, but no significant periodontal probing. Because of the strategic nature of the tooth as a bridge retainer and the presence of swelling, an Oschenbein-Luebke flap was reflected in an effort to evaluate the situation. A fenestration was visualized in association with the apical third of the root. An apicoectomy was performed, including the removal of the silver point and root resection. Staining with methylene blue and transillumination did not reveal any fracture lines. I am hopeful, but believe the prognosis of this tooth is guarded. Anytime you have a history of trauma there is a concern about root fracture.