Throughout my day, I consider the balance of risk and benefit for patients in attempting to help them resolve their dental problems. In the case below, I needed to resolve a case of post treatment disease.
Approximately 10 years ago, nonsurgical root canal therapy was performed on tooth #3.

The patient presented with the following diagnosis on tooth #3: Previously treated, Acute Apical Abscess. This clinical case was characterized by a painful, localized swelling and sinus tract that appeared to be associated with the mesiobuccal root. After talking about the available options, the patient elected nonsurgical retreatment. Our discussion included the risk and benefit of apicoectomy, dental implant therapy and the prognosis of the tooth if treated through surgical or nonsurgical means. I also talked about the possible etiologies of the current condition, the most likely of which was a second, untreated mesiobuccal canal.
Years ago, I was taught that when a root canal needed to be revised, it was best to retreat all of the canals while you were already inside of the tooth. This was presented as dogma, and given the vast amount of knowledge we are taught during dental school, it was an idea that I did not challenge at the time. One of the benefits of experience is that if you continue to think critically, you have an opportunity to continue to grow. A benefit of this growth is that you may have the opportunity to take ideas you were taught and expand on them.
Surgical treatment is usually titrated, meaning when an area is detected radiographically, it is then verified upon surgical access and treatment is rendered solely upon the affected area. Apicoectomies are routinely performed on a single root, ignoring the consideration of the convenience of surgical access in treating the other roots. This is reasonable, as it would be unwise to unnecessarily damage the bone and root of a tooth unaffected by a disease process. In contrast, the aforementioned traditional thinking with regards to nonsurgical retreatment does not consider the restorative risks of retreating all of the canals arbitrarily vs. retreatment of the mesiobuccal root alone. Specifically in this case, the patient presented with acute symptoms that we can use as a reliable bellwether of the disease state. My plan was to start retreatment on the mesiobuccal root, seeking a second mesiobuccal canal. If this did not resolve the patients symptoms, we retain the option to expand the access and retreat the other two canals.
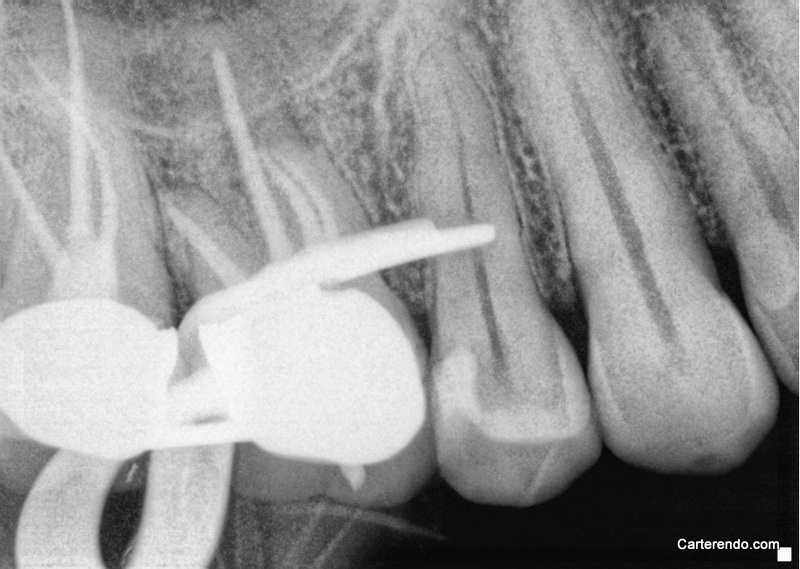
Upon access, we were able to isolate a second mesiobuccal canal, retreat both MB canals and dress both MB canals with Calcium hydroxide. In an effort to visualize the anatomy present, a cone fit was taken prior to placing the Calcium Hydroxide.
Patient presented one month later in no distress, with no signs of swelling, alveolar tendeness, sinus tract or pain to percussion. Both canals were obturated and the patient was referred back to the general dentist for access closure. Follow up contact with the patient yielded no signs of periapical or pulpal disease.

As Endodontists, we are charged with assisting patients in retaining teeth. On a day to day basis I see structural failure of teeth as the overwhelming cause of tooth loss after endodontic treatment. The wise clinican recognizes that our acts as well as our omissions may assist our patients in retaining their teeth for many years to come.
But that can only happen if we use our heads for something other than a hat rack.